The placement of dental implants on an atrophic alveolar ridge is still considered a challenging procedure due to poor bone quantity and quality. Numerous surgical procedures—including guided bone regeneration (GBR), block bone grafting, distraction osteogenesis, and sandwich osteotomy with an interpositional bone graft—have been utilized to overcome vertical bone deficiency.1 GBR is relatively simple compared to a complicated augmentation procedure using a block bone technique or distraction osteogenesis. To achieve successful bone regeneration using the GBR procedure, stability of the particulate bone graft under a resorbable or nonresorbable barrier membrane is essential.2 Collagen membranes are the most common resorbable barrier membranes used to exclude soft-tissue invasion. However, due to the poor stiffness of resorbable collagen membranes, nonresorbable barriers—such as expanded polytetrafluoroethylene (ePTFE) and titanium mesh—are utilized to achieve more favorable space support in three-dimensional ridge augmentation.
The main disadvantage of a nonresorbable barrier membrane is early exposure, which can cause unfavorable bone generation. Technical difficulties can also occur with nonresorbable barrier-supported GBR when placing the membrane over the bone graft with bone tacks or microscrews, and when removing the membrane after the healing period. Preventing collapse of bone grafting placed on the advanced vertical defect is critical for successful reconstitution of a three-dimensional bony defect.
To minimize resorption of bone grafting, it is also necessary to overgraft the bone graft and place titanium screws on the large vertical defects as tenting poles.3 The tent-pole technique is a relatively simpler and less invasive augmentation procedure compared to other augmentation techniques using block bone or titanium mesh. However, the tent-pole technique requires a long edentulous period and an increased number of surgeries, because implants can’t be placed at the same time when performing tent-pole-assisted ridge augmentation.
To overcome these complications, a simplified ridge augmentation procedure using “sticky bone” and tenting abutments was introduced in 2010. In contrast to the screw tenting-pole technique, a tenting abutment technique is performed simultaneously when placing implants on the bony defect. The number of surgeries is reduced, and the edentulous healing period is shortened. In addition, the tenting abutment placed on the implant and the sticky bone prevents collapse of the bone graft and minimizes resorption of the graft during healing, as shown in this case report.
Case report
A 65-year-old female patient visited our department complaining of a masticatory difficulty on the lower right, posterior edentulous ridge. She wanted an implant-supported fixed restoration.
A preoperative radiograph indicated severe horizontal and vertical alveolar defects in the edentulous area.
The surgical procedure was performed under local anesthesia after IV administration of preoperative antibiotics (flomoxef, Flumarin, Ildong Pharmaceutical, Korea) on March 29, 2019. Next, 1.5 cc porcine bone (BONE-XP, Medpark, Busan, Korea) was mixed with autologous fibrin glue (AFG) to make sticky bone as described by Sohn et al.4 A full-thickness flap was retracted to expose the alveolar bone. Underosteotomy was applied to obtain initial stability of the implants. Two 5.0 mm-high x 7.5 mm-wide implants (Biotem dental implants, Biotem Implant Company, Busan, Korea) were placed on the first and second molar areas with good initial stability. One 4.5 mm-wide x 10 mm-high implant was placed on the second premolar site with good stability. The stability of all implants recorded 50 Ncm.
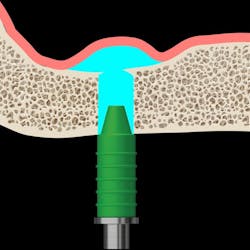
All implant platforms were placed 1 mm subcrestal to the adjacent proximal bone height. Severe three-dimensional bony deficiency was evident around the implants. Three 2 mm-high tenting abutments (SANTA, Biotem Implant Company, Busan, Korea), used as a tenting pole, were placed on the implant platform to maintain the volume of the sticky porcine bone graft during the healing period. The prepared sticky porcine bone graft was grafted on the exposed implant surface and the bony defect for three-dimensional ridge augmentation, respectively. A resorbable collagen membrane (Colla-D, Medpark, Busan, Korea) was used to cover the bone graft without bone tacks. Tension-free sutures were done through the use of a periosteal-releasing incision.
Healing was uneventful before the uncovering procedure. On June 28, 2019, after a three-month healing period, an apically repositioned flap was used to expose the implants and the augmented ridge. A favorable three-dimensional augmentation was achieved. A final zirconia-based restoration was completed after five months’ loading of the provisional restoration (figures 1–5).





Synopsis of Dr. Sohn’s presentation at the Academy of Osseointegration’s 2020 Annual Meeting
Atrophic alveolar bone with a huge defect is a challenging site in which to perform a dental-implant-supported restoration. Various complicated surgical techniques—including autogenous block bone grafting, distraction osteogenesis, and guided bone regeneration using a nonresorbable barrier—have been introduced to achieve favorable bone volume in order to place implants. However, the drawbacks of these techniques are well-known. To overcome the disadvantages of these complicated techniques, a new, innovative surgical technique using sticky bone was introduced in 2010. Dr. Sohn will cover minimally invasive ridge augmentation using sticky bone and tenting abutments during his presentation. Attendees will understand simple surgical management for advanced ridge augmentation.
For more information about the Academy of Osseointegration’s 35th Annual Meeting in Seattle, March 18–21, 2020, including speakers and activities, visit ao2020.osseo.org.
Author's note: Dental professionals can hear Dr. Sohn’s full presentation on this topic, “Simplified Surgical Management Using Sticky Bone for Advanced Ridge Augmentation,” by attending the Academy of Osseointegration’s 2020 Annual Meeting. The meeting, “Evolving Technologies in Implant Dentistry,” will be held March 18–21, 2020, at the Washington State Convention Center in Seattle, Washington. Dr. Sohn will present his topic during the Academy's Surgical Track—Technology for Bone Augmentation on Friday, March 20. Advance registration is available through February 24. For all the meeting details, including online registration, please go to https://ao2020.osseo.org/.
References
1. Tolstunov L, ed. Vertical Alveolar Ridge Augmentation in Implant Dentistry: A Surgical Manual. Hoboken, NJ: John Wiley & Sons Inc.; 2016:161-177.
2. Wang HL, Boyapati L. "PASS" principles for predictable bone regeneration. Implant Dent. 2006;15(1):8-17. doi:10.1097/01.id.0000204762.39826.0f.
3. Le B, Rohrer MD, Prasad HS. Screw "tent-pole" grafting technique for reconstruction of large vertical alveolar ridge defects using human mineralized allograft for implant site preparation. J Oral Maxillofac Surg. 2010;68(2):428-435. doi:10.1016/j.joms.2009.04.059.
4. Sohn DS, Huang B, Kim J, Park WE, Park CC. Utilization of autologous concentrated growth factors (CGF) enriched bone graft matrix (sticky bone) and CGF-enriched fibrin membrane in implant dentistry. The Journal of Implant & Advanced Clinical Dentistry. 2015;7(10):11-29.
Editor’s note: This article originally appeared in Perio-Implant Advisory, a chairside resource for dentists and dental hygienists for issues relating to periodontal and implant medicine. Exclusive content from an academic perspective centers on complex care, solving clinical complications from a team-based approach through interdisciplinary management.