Implant survival rates versus complications
One of the indications for replacing a tooth with a guarded prognosis in need of prosthetic rehabilitation is that the patient has a high caries rate. While replacement of natural teeth with dental implants has a high survival rate, complications can still occur. One systematic review of the literature showed implant survival rates to be 94% after five years and 86% after 10 years. (1) These studies, however, do not take into account complications or failures that can occur on teeth adjacent to the implant.
Teeth migration and open spaces
Recently, implant complications caused by continued craniofacial development after the implant has integrated have been discussed in the literature. One of those complications mentioned is teeth migration of the natural dentition adjacent to an ankylosed implant. It has been suggested that natural teeth adjacent to a dental implant are likely to migrate, especially molars and premolars, in the mesial direction due to continued jaw growth. This migration causes interproximal contact loss (ICL) or an open contact to occur between the implant crown and natural tooth. (2) Studies have indicated that this ICL can occur in 30% to 60% of cases, with an average rate of 52.1% occurring anywhere from three months to 11 years after implant crown insertion. (3) Another study suggests that the mean time for an open contact to occur is around five years postinsertion. (4) Most studies agree that open contacts are more likely to occur on the mesial of the implant crown restoration (78%), as opposed to the distal (22%). (5)
Interproximal contact loss and caries
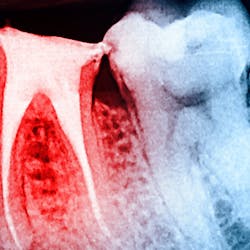
Because ICL between an implant restoration and an adjacent tooth has been highly correlated with the development of caries, a significant health concern arises in individuals with high caries rates who are receiving dental implants (figure 1). Clinicians and allied personnel should be familiar with the factors that contribute to implant-induced decay and are more likely to predispose patients to open contacts. Otherwise, vulnerable patients could be missing out on valuable screening and preventive measures.

Figure 1: Interproximal contact loss between an implant restoration and an adjacent tooth.
4 factors that contribute to implant-induced decay and predispose patients to open contacts:
- An increased Frankfort-mandibular plane angle (FMA) will yield a higher anterior component of force on natural teeth leading to open contacts
- A discrepancy of machine-fit components can lead to translational forces
- The contact addition of a ceramic restoration after firing
- Changes in occlusal force patterns of a patient, especially after the opposing dentition has undergone prosthetic rehabilitation
Monitoring, treatment, and prevention
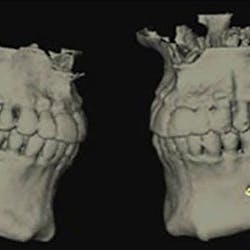
It is imperative for clinicians and teams involved with dental implant care to be aware of implant-induced decay, take necessary radiographs, and perform clinical exams in order to identify open contacts prior to caries development. Once teeth adjacent to implants are afflicted with decay, restoration (figure 2) or even extraction may be warranted (figure 3). To prevent these problems from occurring, individuals who have contributing factors mentioned in this article may benefit from having a screw-retained implant restoration and/or be given an Essix appliance to prevent tooth migration.

Figure 2: This decayed tooth adjacent to an implant requires restoration.

Figure 3: This decayed tooth adjacent to an implant requires extraction.
References
- Lang NP, Berglundh T, Heitz-Mayfield LJ, Pjetursson BE, Salvi GE, Sanz M. Consensus statements and recommended clinical procedures regarding implant survival and complications. Int J Oral Maxillofac Implants. 2004;19(suppl):150-154.
- Greenstein G, Carpentieri J, Cavallaro J. Open contacts adjacent to dental implant restorations: Etiology, incidence, consequences, and correction. J Am Dent Assoc. 2016;147(1):28-34. doi:10.1016/j.adaj.2015.06.011
- Pang NS, Suh CS, Kim KD, Park W, Jung BY. Prevalence of proximal contact loss between implant‐supported fixed prostheses and adjacent natural teeth and its associated factors: a 7‐year prospective study. Clin Oral Implants Res. 2017;28(12):1501-1508. doi:10.1111/clr.13018
- Wei H, Tomotake Y, Nagao K, Ichikawa T. Implant prostheses and adjacent tooth migration: preliminary retrospective survey using 3-dimensional occlusal analysis. Int J Prosthodont. 2008;21(4):302-304.
- Varthis S, Randi A, Tarnow DP. Prevalence of interproximal open contacts between single-implant restorations and adjacent teeth. Int J Oral Maxillofac Implants. 2016;31(5):1089-1092. doi:10.11607/jomi.4432