A protocol for detecting atherosclerosis in the dental office
Key Highlights
- Dental professionals can help detect silent atherosclerotic cardiovascular disease by incorporating the ankle-brachial index (ABI) into routine care, especially for patients with shared risk factors such as diabetes and smoking.
- The ABI is a simple, in-office screening tool with high specificity (98%) and strong sensitivity (around 90%) for identifying significant arterial plaque and peripheral artery disease.
- A clear step-by-step protocol—measure, calculate, interpret, and refer—allows dental teams to support early cardiovascular risk detection while reinforcing the need for medical follow-up.

Author’s note: This test is not a replacement for your physician.
It is increasingly important for dental care providers to understand how to measure the ankle-brachial index (ABI), because atherosclerotic cardiovascular disease (ASCVD) continues to rise globally and often progresses silently. Over the past two decades, cardiovascular deaths have increased from approximately 14 million in 2000 to nearly 19.2 million in 2022, representing 32% of all global deaths with overall cardiovascular disability, and mortality rising by more than 20% during that period.1
In parallel, the global prevalence of atherosclerotic conditions—including ischemic heart disease, ischemic stroke, and peripheral artery disease (PAD)—has steadily increased, affecting over 200 million individuals worldwide.2 PAD, which can be efficiently screened using the ABI, is a well-established marker of systemic atherosclerosis and a strong predictor of myocardial infarction, stroke, and cardiovascular death.
This has direct relevance to dentistry: epidemiologic data show that many adults see a dentist at least once—and often twice—per year, and millions report visiting a dentist but not a physician within the same time frame.3 As oral health-care providers, especially periodontists, who routinely manage patients with shared risk factors such as diabetes, smoking, and chronic inflammation, dental care providers are uniquely positioned to identify vascular risk early. If subclinical atherosclerosis is detected through ABI screening and appropriate referral is made, preventive interventions—including lipid control, antihypertensive therapy, antiplatelet management, and lifestyle modification—may be initiated before a catastrophic cardiovascular event occurs.
The ankle-brachial index is an interesting method for assessing plaque buildup in arteries as it is not only simple to perform at home and in the dental office but also has a high degree of specificity for detecting significant plaque buildup. According to a review, the ABI test boasts a 98% specificity and around 90% sensitivity for detecting significant blockages (50% or greater).4 However, it's important to note that these numbers might be lower for smaller amounts of plaque and for individuals with diabetes, who tend to have lower specificity.
While this test is easy to perform, it's not a substitute for professional medical diagnosis. The ABI test works by measuring resistance in the arteries. Open arteries have little resistance to blood flow, but as plaque builds up, resistance increases. This resistance translates to blood pressure changes, which the ABI test can detect, particularly when there is significant plaque buildup.
To perform the ABI test, follow these three steps:
- Rest for five minutes before starting to ensure accurate blood pressure readings.
- Measure the systolic (top number) blood pressure in both arms and both ankles using an at-home blood pressure monitor.
- Divide the highest systolic number from your ankle measurements by the highest systolic number from your arm measurements.
For example, if your left arm blood pressure is 126/72, left ankle is 128/74, right arm is 130/78, and right ankle is 124/76, you'll use the systolic numbers: 128 (ankle) and 130 (arm). Dividing these gives you 0.98.
By using this test, the dental care provider can gain valuable insights into the patient’s cardiovascular health, but remember to always refer to a physician for a comprehensive diagnosis and treatment plan. Because while the ABI can detect serious arterial plaque, it is less sensitive to mild arterial plaque, especially when doing it at home/in office compared to with a cardiologist.
Steps for the ABI test
You will need an automatic blood pressure cuff.
Step 1: Rest
Before beginning, have a blood pressure monitor/cuff and something to take notes with you. Have your patient sit quietly for five minutes. They should not have consumed any stimulants.
Step 2: Blood pressure measurement
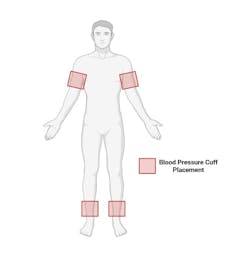
Have the patient lie down and put the blood pressure cuff on each of these locations: left upper arm, right upper arm, slightly above left ankle, slightly above right ankle (see figure 1 for location guidance), and measure the blood pressure in a rested manner. Write all the results down; you should have a top number (systolic blood pressure) and a bottom number (diastolic blood pressure) for each measurement.
Step 3: Calculating results
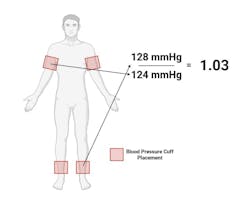
- Of all the values you have measured, select the highest systolic (top number) blood pressure for one arm measurement (left or right) and one ankle measurement (left or right).
- Divide the ankle number by the arm number (see figure 2 for guidance).
- This is your ankle-brachial index.
Step 4: Interpreting the results
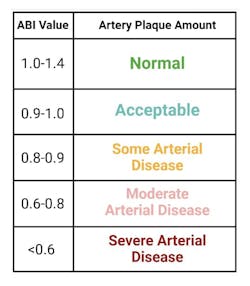
Interpret the results using figure 32:
- 9 to 1.4: Likely no significant plaque buildup
- 6 to 0.89: Possible plaque buildup
- Below 0.6: High likelihood of significant plaque buildup
Additionally, there is a more sensitive test for detecting plaque, but it requires more planning. If you're interested, follow this step-by-step guide along with a plethora of resources on cardiovascular health.
Immediate steps if your ABI value is between 0.8 and 0.89 should include focusing on reducing cardiovascular disease risks, such as managing blood pressure, cholesterol, weight, and insulin resistance. Values below 0.8 warrant a thorough evaluation by a physician and confirmation testing.
Step 5: Acting on the results
Use figure 4 for possible actions based on the results of the ABI.
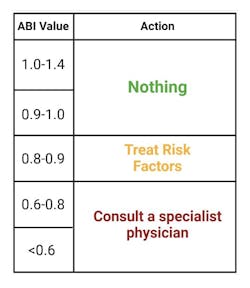
Risk factor reductions include reducing blood pressure, reducing cholesterol-containing lipoproteins, improving HbA1C and HOMA-IR (measures of insulin resistance), weight loss, and so on.
Conclusion
The ABI is designed to detect atherosclerosis (plaque) in the arteries. It is specific and accurate for people with over 50% blockage of their arteries, but less effective for people with less than 50% blockage (although it may still reveal results). This article is a step-by-step guide on how to detect atherosclerosis using the ABI test, what the results mean, and how to proceed.
Please keep in mind that the exactness of this test is also dependent on the implementation accuracy, so this shouldn’t be a one-stop diagnosis but used as additional information in your patient’s health journey. Also, if you have values that are borderline, it may be worthwhile to check in with your physician regardless to be safe and account for possible measurement error.
Editor’s note: This article originally appeared in Perio-Implant Advisory, a chairside resource for dentists and hygienists that focuses on periodontal- and implant-related issues. Read more articles and subscribe to the newsletter.
References
- Cardiovascular diseases (CVDs). World Health Organization. July 31, 2025. https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds)
- Allison MA, Armstrong DG, Goodney PP, et al. Health disparities in peripheral artery disease: a scientific statement from the American Heart Association. Circulation. June 15, 2023. https://www.ahajournals.org/doi/10.1161/CIR.0000000000001153
- Manski R, Rohde F, Ricks T. Trends in the number and percentage of the population with any dental or medical visits, 2003-2018. Agency for Healthcare Research and Quality. October 2021. https://meps.ahrq.gov/data_files/publications/st537/stat537.pdf
- Patel Y, Shah A, Patel P, et al. Diagnostic accuracy of ankle-brachial index in patients with peripheral arterial disease: a meta-analysis. Cardiol Rev. 2025. doi:10.1097/CRD.0000000000001085
About the Author
Nicolas Verhoeven, PhD
Nicolas Verhoeven, PhD, is owner and content creator for Physionic. He has a PhD in molecular medicine/cell and molecular physiology and an MS in exercise physiology. He has been a cell and molecular biology researcher for 10 years and is a professor of physiology in nutrition.

Scott Froum, DDS
Editorial Director
Scott Froum, DDS, a graduate of the State University of New York, Stony Brook School of Dental Medicine, is a periodontist in private practice at 1110 2nd Avenue, Suite 305, New York City, New York. He is the editorial director of Perio-Implant Advisory and serves on the editorial advisory board of Dental Economics. Dr. Froum, a diplomate of both the American Academy of Periodontology and the American Academy of Osseointegration, is in the fellowship program at the American Academy of Anti-aging Medicine, and is a volunteer professor in the postgraduate periodontal program at SUNY Stony Brook School of Dental Medicine. He is a trained naturopath and is the scientific director of Meraki Integrative Functional Wellness Center. Contact him through his website at drscottfroum.com or (212) 751-8530.