A comparison of graft techniques for the alveolar ridge prior to oral implant
Success of a dental implant can be affected by the width of the alveolar ridge — an indication of the amount of bone available to hold the implant. A variety of methods exist, each with their own advantages, to determine bone loss and subsequent augmentation techniques. The ridge-split graft is highlighted as a strategy for treating horizontally collapsed alveolar ridges. The Journal of Oral Implantology offers a comparison of two commonly used techniques, the ridge-split and the block bone grafts. The oral surgeon must choose the best technique for bone augmentation based on an assessment of the patient’s condition and the oral surgeon’s own skills and experience.
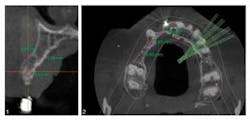
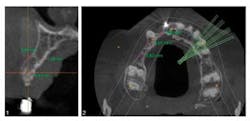
Diagnosis of alveolar bone should first be assessed visually for width and height and the relationships of teeth to one another and to the dental arch. Radiographic images can distinguish two-dimensional versus three-dimensional bone deficiency. A three-dimensional or volumetric bone evaluation with cone-beam computed tomography allows for precise measurement of the ridge and evaluation of both the cortical and medullary portion of the bone, which are imperative for the stability of the implant. A 10-point comparison of the two graft techniques, ridge-split and block bone, is offered within this article. Issues discussed include graft resorption, donor and recipient site morbidity, wound closure, buccal soft tissue flap, immediate or delayed implant insertion, and long-term stability of the graft. Both methods are used primarily for horizontal alveolar ridge augmentation, or bone widening. Block bone grafting is effective for severe anterior atrophy in the upper and lower jaw. However, morbidity at the donor site and later-term graft resorption can occur with this method. Some advantages of the split-ridge procedure include the lack of a donor site and that the buccal flap is not compromised but left attached. A postoperative injury while chewing is less likely with the ridge-split method because the graft is positioned more internally, protecting the area. While the choice of graft technique must ultimately be decided by the experience and comfort level of the operator, the author asserts that the ridge-split treatment has many advantages and produces a stable graft over time. Full text of the article, “Classification of the Alveolar Ridge Width: Implant Driven Treatment Considerations for the Horizontally-Deficient Alveolar Ridges,” Journal of Oral Implantology, Vol. 40, Special Issue 1, 2014, is available here. For more information about Journal of Oral Implantology, visit their website.ADDITIONAL READING ...Study finds that shorter waiting time between dental procedures is adequateAtrophic patients have more options with new dental implantLess invasive approach to dental implants allows heart patients to continue anticoagulation therapy