Modifications to platelet-rich fibrin (PRF): From resorption of 2 weeks to 4-6 months utilizing the novel Bio-Heat technology
Key Highlights
- Bio-Heat technology transforms traditional PRF into extended PRF (e-PRF), increasing membrane resorption time from two to three weeks to as long as four to six months.
- e-PRF combines heated albumin gel with concentrated PRF to create a longer-lasting, biologically active membrane for guided bone regeneration, extraction sites, sinus grafting, and recession coverage.
- Beyond dentistry, injectable e-PRF shows promise as a natural alternative to synthetic dermal fillers and as a regenerative treatment for joint, cartilage, and sports-related injuries.

Abstract
Platelet-rich fibrin (PRF) has been demonstrated to be an excellent biomaterial addition to most surgeries performed in dentistry owing to its excellent biocompatibility, supraphysiological concentration of autogenous cells and regenerative growth factors over time. Nevertheless, one of the main reported drawbacks of PRF is its rather fast resorption properties characterized within a two-to-three-week time frame, thus limiting its use as a “barrier: membrane in GBR/GTR procedures.
Interestingly, recent studies have demonstrated that by heating a liquid platelet-poor plasma (PPP) layer, the resorption properties of heated albumin (albumin gel) could be significantly extended from a standard two-week resorption period to greater than four months (extended-PRF; e-PRF) using the Bio-Heat technology.
This brief overview highlights the scientific development over the past five years utilizing this novel regenerative modality demonstrating its marked improvement in membrane stability. These e-PRF membranes have since been utilized as a biological barrier membrane for GBR, extraction site management, root coverage, and closure of the lateral window during sinus grafting procedures with a longer-lasting half-life. This article also briefly discusses its use in regenerative medicine as a biological filler material that can be utilized as a replacement for synthetic fillers such as Juvéderm and Restylane in esthetic medicine applications and as a regenerative agent in sports medicine for damaged cartilage such as knees and shoulders.
Introduction
Platelet concentrates have been utilized in many fields of regenerative medicine for over three decades1 owing to their ability to deliver supraphysiological concentrations of autologous platelets, leukocytes, and growth factors.2,3 While platelet-rich plasma (PRP) has been extensively employed as a first-generation platelet concentrate, platelet-rich fibrin (PRF) has since been utilized with a better ability to release more growth factors over an extended period of time with superior clinical outcomes in various fields of medicine and dentistry.4,5 PRF has proven to be an excellent biomaterial composed of autogenous cells and growth factors entrapped within a fibrin network that have been shown to break down more slowly over time when compared to traditional PRP.5
Nevertheless, one of the main reported drawbacks of PRF (and especially PRP) is its faster-than-ideal resorption rate characterized within a two-to-three-week time frame.6 Because of its fast resorption rate, PRF membranes cannot be utilized as a barrier membrane similar to collagen due to their inability to exclude soft tissues over an extended period of time. Interestingly, a number of recent studies have demonstrated that PRF could be significantly extended from two-to-three-week resorption properties to greater than four months (extended-PRF; e-PRF) by heating a liquid platelet-poor plasma (PPP) layer (denaturing albumin) using Bio-Heat technology.7
This heated version of platelet poor plasma (PPP), which has now been utilized in many areas of medicine and dentistry, has recently been the basis of intensive research endeavors across many regenerative labs owing to its extended working properties. Since one of the main limitations of PRP/PRF has historically been its short in vivo turnover rate, these extended PRF membranes can be used as substitutes for collagen membranes in various bone regeneration applications requiring a typical “barrier” function that protects bone regeneration from faster growing soft tissues.8
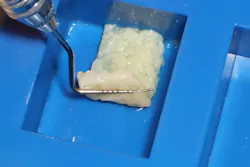
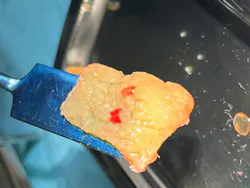
To overcome the quick degradation properties of platelet concentrates and better maintain volume stability, the Alb-PRF protocol was developed. This protocol involves the use of the PPP layer (containing ~60% albumin) and heating it to 75 °C for 10 minutes to allow for albumin denaturation as well as breaking of many weak linkages or bonds (e.g., hydrogen bonds) within its protein molecule. Following denaturation, the proteins are then restructured in a more densely organized assembly that extends the resorption properties of PRF to up to four to six months (QR code 1).9-12 However, the heating process also destroys cells/growth factors, and thereby, the platelet concentrates lose much of their regeneration potential. For these reasons and following heating, a concentrated PRF layer (C-PRF)13,14 taken from the buffy coat is then mixed back into the heated PPP (albumin gel) once cooling has occurred (termed Alb-PRF or e-PRF for extended PRF).15

In view of previous research to date on this topic, the aim of this short review article is to present the biological properties of this novel regenerative modality. Furthermore, the step-by-step processing of e-PRF as well as clinical studies to date on the topic is presented in Figure 1. As an injectable filler, a 25G needle or 22G canula is recommended (QR code 2). Alternatively, a similar process can be utilized to create a custom shape membrane with extended properties (e-PRF) lasting up to four months and utilized clinically as a substitute for collagen membranes (figure 2, QR code 3).




Clinical use of Alb-PRF/e-PRF membranes for periodontology and implant dentistry
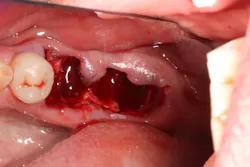
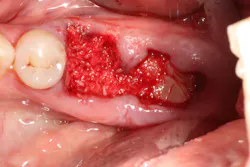
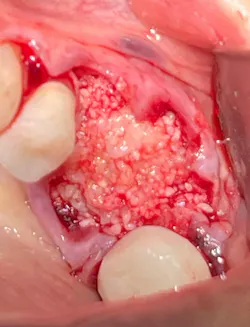
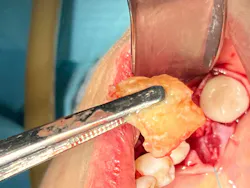
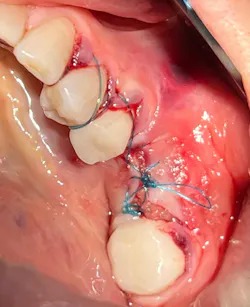
One of the main areas where the e-PRF membranes were first clinically utilized and tested was as a substitute for collagen membranes (QR code 1). Therefore, several clinical case series were started whereby the e-PRF membranes were created and utilized for extraction site management to cover bone allografts following tooth removal similar to either a collagen membrane/plug or a PTFE membrane (figure 3). This opportunity offers clinicians a 100% all-natural biomaterial with extended resorption properties that can also be left exposed in the oral cavity following placement. Notably, the e-PRF membranes may also be left exposed in the oral cavity, and their inclusion of supraphysiological concentrations of leukocytes allows for greater defense against incoming pathogens16 as well as lead to less pain postoperatively.17 QR code 4 highlights a clinical example of an e-PRF membrane used, and Figure 3F highlights the much faster soft tissue closure ability of epithelial tissue over the e-PRF membrane when compared to alternative strategies.

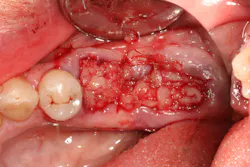



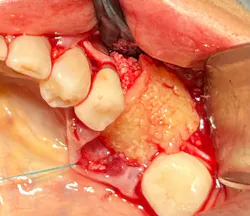
E-PRF membranes have been utilized extensively during GBR procedures (figure 4, QR code 5). Here, such membranes may be much less foreign to soft tissues, with reports of improved biocompatibility. Finally, e-PRF membranes have also been utilized as a substitute for various collagen membranes during recession coverage procedures utilizing a vestibular tunneling approach (figure 5, QR code 6).











In summary, clinical studies have now utilized the e-PRF membranes in various applications similar to collagen barrier membranes (as their replacement) for procedures including ridge preservation,18-21 intrabony defect regeneration,22, 23 bone regeneration,24 papilla reconstruction,25 immediate dental implant placement,26 sinus grafting,27,28 third molar extraction,29 and recession coverage.30
Clinical studies using e-PRF as an injectable bio-filler in esthetic and sports medicine
To date, thousands of cases have utilized the technology of extending the working properties of platelet concentrates as a biological filler (Bio-Filler). One of the first approaches was to restore the facial volume (figure 6, QR code 7).31 Interestingly, Alb-PRF has also been utilized for injections into deficient papilla with quite promising results, yielding up to four years of data (figure 7, QR code 8). Last, Alb-PRF has also been utilized as a biological growth factor for joint and spinal injections such as diseased osteoarthritic joints and spinal injections (QR code 9).32-35









- Use of horizontal centrifugation of platelet-rich fibrin leads to a 4-fold increase in cell concentration
- Potential applications of exosomes in medicine and dentistry
- The use of exosomes to save teeth
Editor’s note: This article originally appeared in Perio-Implant Advisory, a chairside resource for dentists and hygienists that focuses on periodontal- and implant-related issues. Read more articles and subscribe to the newsletter.
References
- Miron RJ, Estrin NE, Ahmad P, et al. Thirty years of autologous platelet concentrates: from platelet-rich plasma to platelet-rich fibrin. J Periodont Res. 2025. Published online: August 4, 2025. doi:10.1111/jre.70013
- Miron RJ, Fujioka-Kobayashi M, Bishara M, Zhang Y, Hernandez M, Choukroun J. Platelet-rich fibrin and soft tissue wound healing: a systematic review. Tissue Eng Part B Rev. 2017;23(1):83-99. doi:10.1089/ten.TEB.2016.0233
- Miron RJ, Zucchelli G, Pikos MA, et al. Use of platelet-rich fibrin in regenerative dentistry: a systematic review. Clin Oral Investig. 2017;21(6):1913-1927. doi:10.1007/s00784-017-2133-z
- Fujioka-Kobayashi M, Miron RJ, Hernandez M, Kandalam U, Zhang Y, Choukroun J. Optimized platelet-rich fibrin with the low-speed concept: growth factor release, biocompatibility, and cellular response. J Periodontol. 2017;88(1):112-121. doi:10.1902/jop.2016.160443
- Kobayashi E, Flückiger L, Fujioka-Kobayashi M, et al. Comparative release of growth factors from PRP, PRF, and advanced-PRF. Clin Oral Investig. 2016;20(9):2353-2360. doi:10.1007/s00784-016-1719-1
- Fujioka-Kobayashi M, Schaller B, Mourão C, Zhang Y, Sculean A, Miron RJ. Biological characterization of an injectable platelet-rich fibrin mixture consisting of autologous albumin gel and liquid platelet-rich fibrin (Alb-PRF). Platelets. 2021;32(1):74-81. doi:10.1080/09537104.2020.1717455
- Gheno E, Mourão CFdAB, Mello-Machado RCd, et al. In vivo evaluation of the biocompatibility and biodegradation of a new denatured plasma membrane combined with liquid PRF (Alb-PRF). Platelets. 2021:32(4):542-554. doi:10.1080/09537104.2020.1775188
- Kawase T, Kamiya M, Kobayashi M, et al. The heat-compression technique for the conversion of platelet-rich fibrin preparation to a barrier membrane with a reduced rate of biodegradation. J Biomed Mater Res B Appl Biomater. 2015;103(4):825-831. doi:10.1002/jbm.b.33262
- Jung SY, Kim HY, Oh HJ, Choi E, Cho MS, Kim HS. Feasibility of autologous plasma gel for tonsil-derived stem cell therapeutics in hypoparathyroidism. Sci Rep. 2018;8(1):11896. doi:10.1038/s41598-018-30454-1
- Doghaim NN, El-Tatawy RA, Neinaa YME. Assessment of the efficacy and safety of platelet poor plasma gel as autologous dermal filler for facial rejuvenation. J Cosmet Dermatol. 2019;18(5):1271-1279. doi:10.1111/jocd.12876
- Mourão CFdAB, Gheno E, Lourenço ES, et al. Characterization of a new membrane from concentrated growth factors associated with denaturized Albumin (Alb-CGF) for clinical applications: a preliminary study. International Journal of Growth Factors and Stem Cells in Dentistry. 2018;1:64.
- Garg A. Autologous Platelet Concentrates. Quintessence; 2018:188.
- Miron RJ, Chai J, Zhang P, et al. A novel method for harvesting concentrated platelet-rich fibrin (C-PRF) with a 10-fold increase in platelet and leukocyte yields. Clin Oral Investig. 2020;24(8):2819-2828. doi:10.1007/s00784-019-03147-w
- Fujioka-Kobayashi M, Katagiri H, Kono M, et al. Improved growth factor delivery and cellular activity using concentrated platelet-rich fibrin (C-PRF) when compared with traditional injectable (i-PRF) protocols. Clin Oral Investig. 2020;24(12):4373-4383. doi:10.1007/s00784-020-03303-7
- Fujioka-Kobayashi M, Schaller B, Mourão CFDAB, Zhang Y, Sculean A, Miron RJ. Biological characterization of an injectable platelet-rich fibrin mixture consisting of autologous albumin gel and liquid platelet-rich fibrin (Alb-PRF). Platelets 2021;32(1):74-81. doi:10.1080/09537104.2020.1717455
- Moraschini V, Miron RJ, Mourao CFdAB, et al. Antimicrobial effect of platelet‐rich fibrin: a systematic review of in vitro evidence‐based studies. Periodontol 2000. 2024;94(1):131-142. doi:10.1111/prd.12529
- Estrin NE, Tran TB, Ahmad P, et al. Analgesic effects of platelet-rich fibrin (PRF): a systematic review. Periodontol 2000. 2025. Published online: October 13, 2025. doi:10.1111/prd.70014
- Moualla Z, Qasem T, Alnada A. Alveolar ridge preservation using a mixture of Alb‐PRF and alloplastic bone graft: a case report. Case Rep Dent. 2025;2025:3007346. doi:10.1155/crid/3007346
- Estrin NE, Espinoza AR, Ahmad P, Imber J-C, Farshidfar N, Miron RJ. The evolution of extended platelet-rich fibrin membranes for socket grafting: part one: technical development of protocols. Dent J. 2025;13(12):604. doi:10.3390/dj13120604
- Estrin NE, Tran TB, Espinoza AR, et al. Safety and feasibility of extended platelet‐rich fibrin as a solo barrier membrane for ridge preservation: a case series. Clin Exp Dent Res. 2026;12(1):e70282. doi:10.1002/cre2.70282
- Estrin NE, Ahmad P, Tran TB, et al. The evolution of extended platelet-rich fibrin membranes for socket grafting: part two: a randomized clinical trial comparing these membranes with collagen membranes. Dent J (Basel). 2026;14(1):45. doi:10.3390/dj14010045
- Kumari S, Sharma AK, Sunil MKS, Koppula SK, Sharma S. A randomized controlled study comparing albumin-enriched platelet-rich fibrin and conventional platelet-rich fibrin for the treatment of intrabony defects. J Pharm Bioallied Sci. 2025;17(Suppl 2):S1619-S1621. doi:10.4103/jpbs.jpbs_190_25
- Shirakata Y, Sena K, Nakamura T, et al. Histological evaluation of gingival and intrabony periodontal defects treated with platelet-rich fibrin using different protocols: a canine study. Oral Health Prev Dent. 2021;19:537-546. doi:10.3290/j.ohpd.b2182985
- Shokry MMEM, Melek LNF, Amer TA. Three-dimensional volumetric analysis of bone regeneration following jaw cyst enucleation with and without an autologous albumin gel-platelet-rich fibrin mixture (Alb-PRF): a randomized controlled clinical trial. BMC Oral Health 2025;25(1):693. doi:10.1186/s12903-025-06027-w
- Saberi BV, Sigaroudi AK, Kamani M, Rafiei E. Comparison of the effect of albumin with platelet-rich fibrin (Alb-PRF) gel and hyaluronic acid gel injection on interdental papilla reconstruction: a randomized clinical trial. J Adv Periodontol Implant Dent. 2024;16(2):109-115. doi:10.34172/japid.2024.018
- Alsabahi H, Mowafey B, Kandil I, Elgohary N, Youssef J. Clinical and radiographic evaluation of autologous albumin-rich platelet-rich fibrin membrane versus synthetic collagen membrane for immediate dental implant placement in the maxillary esthetic zone: a preliminary randomized clinical trial. BMC Oral Health 2026;26(1):292. doi:10.1186/s12903-026-07683-2
- Barakat M, Khalil A, Albash Z. Efficacy of platelet-rich albumin and fibrin gel in two-stage lateral sinus lift: a prospective study. Ann Med Surg (Lond). 2025;87(9):5409-5416. doi:10.1097/MS9.0000000000003589
- Estrin NE, Basma H, Espinoza AR, Pinto MAC, Pikos MA, Miron RJ. Extended platelet‐rich fibrin as a membrane for lateral window sinus lifts: a case series. Clin Implant Dent Relat Res. 2025;27(1):e13427. doi:10.1111/cid.13427
- Javid K, Mourão CF, Mello-Machado RC, et al. Clinical and biochemical evaluation of the use of Alb-PRF versus L-PRF in mandibular third molar extractions: a split-mouth randomized clinical trial. J Funct Biomater. 2023;14(1):505. doi:10.3390/jfb14100505
- Abdulhak S, Kassem T, Alsayed Tolibah Y. Comparison between autologous albumin gel and liquid platelet-rich fibrin mixture versus connective tissue graft to modify the gingival phenotype: a randomized controlled trial. Cureus. 2024;16(6):e61958. doi:10.7759/cureus.61958
- Davies C, Miron RJ. Autolougous platelet concentrates in esthetic medicine. Periodontol 2000. 2025;97(1):363-419. doi:10.1111/prd.12582
- Miron RJ, Pikos MA, Estrin NE, et al. Extended platelet‐rich fibrin. Periodontol 2000. 2024;94(1):114-130. doi:10.1111/prd.12537
- Ogéus T. Platelet-rich fibrin in combination with heat coagulated albumin gel as treatment for lateral epicondylitis, a retrospective 1-year follow-up study. J Orthop Sports Med. 2024;6:219-226. doi:10.26502/josm.511500165
- Ogéus T. Treatment of a fractured humerus and partially torn supraspinatus tendon in a professional boxer with liquid platelet-rich fibrin and heat-coagulated albumin gel: a case report. J Med Case Rep. 2024;18(1):124. doi:10.1186/s13256-024-04458-7
- Ogéus T. Treatment of Osgood-Schlatter disease in an adolescent athlete with liquid platelet-rich fibrin and heat-coagulated albumin gel: a case report. Eur J Med Case Rep. 2024;8:53-56. doi:10.24911/ejmcr/173-1701008366
- Fujioka-Kobayashi M, Schaller B, Mourao C, Zhang Y, Sculean A, Miron RJ. Biological characterization of an injectable platelet-rich fibrin mixture consisting of autologous albumin gel and liquid platelet-rich fibrin (Alb-PRF). Platelets. 2021;32(1):74-81. doi:10.1080/09537104.2020.1717455
- Miron RJ. Understanding Platelet Rich Fibrin: Quintessence; 2021.
About the Author

Richard Miron, DDS
Richard Miron, DDS, is currently lead educator and researcher at Advanced PRF Education and an adjunct visiting faculty in the department of periodontology at the University of Bern, Switzerland, where he completed his PhD studies since 2009. Dr. Miron is a prolific author and international lecturer on topics relating to growth factors, bone biomaterials, and guided bone regeneration. He is widely considered one of the top contributors to implant dentistry. He has written 10 textbooks on regenerative dentistry including Next Generation Biomaterials for Bone and Periodontal Regeneration, Understanding Platelet Rich Fibrin, and Modern Implant Dentistry.

Nathan Estrin, DMD
Nathan Estrin, DMD, received his bachelor’s degree in kinesiology from Indiana University and went on to earn his DMD from LECOM School of Dental Medicine. He received his training in periodontics at Stony Brook University in New York. During his dental studies, he developed a passion for regenerative, implant, and laser surgery and has more than 15 publications and three book chapters in these areas. Dr. Estrin is a board-certified periodontist in full-time private practice in Sarasota, Florida. He is also adjunctive faculty at LECOM School of Dental Medicine and a lead educator for PRFedu, where he trains dental offices on platelet-rich fibrin, lasers, and modern periodontal therapy.