Obesity and periodontal disease: Understanding the inflammatory pathway
Key Highlights
- Obesity fuels periodontal inflammation: Visceral fat releases inflammatory cytokines that can accelerate gum disease progression and increase the body's overall inflammatory burden.
- Look beyond BMI: Waist circumference and waist-to-height ratio may better predict periodontal disease risk because they more accurately reflect harmful visceral fat.
- Lifestyle changes support oral health: Regular exercise, improved metabolic health, and maintaining muscle mass can reduce chronic inflammation and complement periodontal therapy for better oral and systemic outcomes.

Obesity and periodontal disease are two of the most prevalent chronic inflammatory diseases worldwide. Current estimates suggest that nearly 47% of US adults are affected by periodontitis, while obesity affects approximately 40% of the population.1,2 Over the past several decades, it has become increasingly clear that the mouth cannot be viewed separately from the rest of the body. A growing body of evidence has demonstrated that oral diseases, particularly periodontal disease, are associated with numerous systemic conditions including diabetes, cardiovascular disease, rheumatoid arthritis, Alzheimer's disease, and obesity. To date, periodontal disease has been linked to more than 70 systemic conditions.3 It is now clear that oral health reflects systemic health, and one has the potential to impact the other. This concept, commonly referred to as the oral-systemic link, has fundamentally changed how we treat periodontal disease.
The link between obesity and periodontal disease
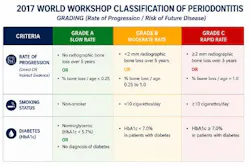
The relationship between obesity and periodontal disease is not a new observation. In fact, the first study to show this relationship was published in 1977, where obese rats demonstrated increased periodontal destruction compared to healthy controls.4 This connection is not particularly surprising. The oral-systemic link is perhaps best highlighted by the well-established relationship between periodontal disease and diabetes. Decades of research have revealed a two-way relationship between these two conditions.5 In fact, the evidence between periodontal disease and diabetes is so strong that in 2017, diabetic status (measured by HbA1c) was actually built into the diagnosis of periodontitis (figure 1). Given the overall metabolic dysfunction of diabetic patients, it is reasonable to assume that obesity may have a similar impact on periodontal disease.
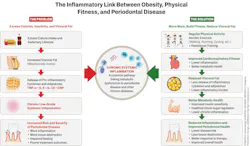
How exactly does obesity influence the health of the gums? The answer appears to lie in chronic inflammation. For many years, adipose tissue (fat) was viewed simply as a passive storage site, filled with excess calories in the form of triglycerides. Today, we know that adipose tissue is biologically active, acting more like an endocrine organ. This means that fatty tissue is constantly releasing different chemical signals and hormones into the bloodstream.
Most notably, it releases pro-inflammatory cytokines, such as TNF-α, IL-6, and IL-1β. As these mediators enter the bloodstream, they amplify the immune response and cause chronic, low-grade systemic inflammation throughout the body. This “hyper-inflamed” state primes the immune system to respond more aggressively to otherwise routine bacterial or immunologic challenges, helping explain why some individuals with obesity experience disproportionately severe periodontal inflammation and tissue breakdown, despite relatively modest accumulations of dental plaque (figure 2).
On a broader scale, this persistent inflammation increases one’s risk of developing other chronic diseases. This can pose serious health concerns, as chronic diseases are the leading cause of death and disability worldwide.7

Importantly, we need to recognize that not all body fat behaves the same. We have learned that different types of fat have vastly different properties. Subcutaneous fat, located directly beneath the skin, primarily serves as an energy reserve and is relatively inactive. In contrast, visceral fat accumulates deep within the abdominal cavity, around organs such as the liver and intestines. Visceral fat is more active than subcutaneous fat and is a major source of inflammatory cytokines that drive chronic inflammation throughout the body.8 To optimize healthy outcomes, it’s clear we need to focus on visceral fat.
Measuring obesity: Beyond BMI
While obesity is commonly discussed in terms of body weight, not all measures of obesity are equally useful. For example, the body mass index (BMI) has long served as the standard screening tool for obesity, in part due to its ease of use (only requiring a person’s height and weight). However, BMI has been widely criticized. For one, it cannot distinguish between muscle mass and fat, let alone different kinds of fat tissue or where they are stored. As a result, two individuals with the same BMI may have markedly different metabolic health and inflammatory burden.
According to recent evidence, measures such as waist circumference, or even better, waist-to-height ratio, may provide a more accurate assessment of overall health and chronic disease risk than BMI alone.9 This is likely because these measurements better reflect the amount of one’s visceral fat, which primarily accumulates in the abdomen. This distinction may be particularly relevant in the management of periodontal disease.
A large 2025 Korean population-based study reported a stronger association between waist circumference and periodontitis compared with BMI, suggesting the key role of fat distribution and visceral fat in periodontal disease risk.10
While the most accurate measurements of visceral fat require advanced imaging or specialized scales, monitoring waist size provides a simple and practical way to mitigate risk of chronic diseases. One widely used approach is the “0.5 rule” for waist-to-height ratio, which was proposed as a global screening guideline for mortality and cardiometabolic risk. Simply put, it’s best to keep your waist circumference to less than half your height. For example, a person who stands 5’6” (66 inches) should aim for a waist circumference of less than 33 inches.
The role of physical fitness
The good news is that the relationship between obesity, periodontal disease, and systemic inflammation is largely modifiable. Metabolic health can be improved, and regular physical activity is one of the most effective ways to manage chronic inflammation throughout the body.11 Exercise has been shown to lower circulating inflammatory markers, reduce visceral fat, and improve insulin sensitivity.12 These changes ultimately reduce the inflammatory burden that is increasingly recognized as a key contributor to both metabolic dysfunction and periodontal disease progression (figure 3). If the effects of exercise could be packaged into a pill, it would likely be the most prescribed drug worldwide.
While aerobic exercise, resistance training, and high-intensity interval training (HIIT) have emerged as the most effective ways to reduce visceral fat, these benefits are not limited to structured exercise programs.13 Evidence clearly shows the benefits of exercise are dose dependent, meaning that even modest increases in daily movement can yield substantial improvements, especially in sedentary or obese individuals.14 For many patients, especially those just beginning their fitness journeys, this may be a more realistic starting point. Tracking daily step count has emerged as a practical and accessible way to quantify activity, providing patients with a simple and tangible goal that can be gradually increased over time. While evidence regarding periodontal disease and fitness is still emerging, several cross-sectional studies have revealed that regular walking and physical activity are associated with a lower prevalence of periodontal disease.15,16
Why muscle matters
While it’s clear that physical activity and reductions in visceral fat are key in reducing chronic inflammation, an often-overlooked piece of the metabolic puzzle is muscle mass. Most people think of skeletal muscle as the tissue responsible for movement and strength, but it is also one of the body's most important metabolic organs. In fact, skeletal muscle accounts for approximately 70%–80% of blood glucose uptake, making it essential for maintaining healthy blood sugar levels and insulin sensitivity.17 When muscle mass is reduced, our ability to regulate blood glucose is impaired, increasing the risk of type 2 diabetes. Since we already know about the strong association between diabetes and periodontal disease, it is logical to suggest that improving metabolism by building muscle is another tool to help keep the mouth (and body) healthy.
Conclusion
As our understanding of the oral-systemic link continues to evolve, future studies will undoubtedly provide greater insight into the complex relationship between chronic inflammation, obesity, and periodontal disease. While bacterial infection and plaque accumulations will remain key factors in the management of periodontal disease, the evidence is clear—we must also view gum disease through a lens of systemic inflammation. Of course, periodontal treatment is still a key to success, including antimicrobial control, surgical or regenerative treatment when necessary, and continued personalized maintenance programs. However, as health care increasingly shifts toward a preventive and integrative model, periodontists are uniquely positioned to play a broader role in promoting overall health. Discussions regarding exercise, metabolic health, nutrition, smoking cessation, and lifestyle modification should not be viewed as separate from periodontal care. Rather, they represent an opportunity to address the chronic inflammatory burden that affects the lives of so many patients.
Most importantly, the hope is to translate our knowledge into functional, personalized care to improve both our patients’ oral and systemic health. With emerging technology and the ability to measure key inflammatory markers, treatment protocols are already being developed to help solve these inflammatory problems. By understanding this connection, periodontists have a chance to create not only healthier mouths, but also longer and healthier lives.
Editor’s note: This article originally appeared in Perio-Implant Advisory, a chairside resource for dentists and hygienists that focuses on periodontal- and implant-related issues. Read more articles and subscribe to the newsletter.
References
- Eke PI, Dye BA, Wei L, et al. Update on prevalence of periodontitis in adults in the United States: NHANES 2009 to 2012. J Periodontol. 2015;86(5):611-622. doi:10.1902/jop.2015.140520
- Hales CM, Carroll MD, Fryar CD, Ogden CL. Prevalence of obesity and severe obesity among adults: United States, 2017-2018. NCHS Data Brief. 2020;(360):1-8.
- Romandini M, Hajishengallis G, Curtis M, Baima G. Periodontal medicine rewired: mechanisms linking periodontitis to systemic diseases. J Periodontal Res. Published online April 19, 2026. doi:10.1111/jre.70099
- Perlstein MI, Bissada NF. Influence of obesity and hypertension on the severity of periodontitis in rats. Oral Surg Oral Med Oral Pathol. 1977;43(5):707-719. doi:10.1016/0030-4220(77)90055-x
- Mealey BL, Oates TW; American Academy of Periodontology. Diabetes mellitus and periodontal diseases. J Periodontol. 2006;77(8):1289-1303. doi:10.1902/jop.2006.050459
- Papapanou PN, Sanz M, Buduneli N, et al. Periodontitis: consensus report of workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J Periodontol. 2018;89(Suppl 1):S173-S182. doi:10.1002/JPER.17-0721
- Hacker K. The burden of chronic disease. Mayo Clin Proc Innov Qual Outcomes. 2024;8(1):112-119. doi:10.1016/j.mayocpiqo.2023.08.005
- Fontana L, Eagon JC, Trujillo ME, Scherer PE, Klein S. Visceral fat adipokine secretion is associated with systemic inflammation in obese humans. 2007;56(4):1010-1013. doi:10.2337/db06-1656
- Ashwell M, Gunn P, Gibson S. Waist-to-height ratio is a better screening tool than waist circumference and BMI for adult cardiometabolic risk factors: systematic review and meta-analysis. Obes Rev. 2012;13(3):275-286. doi:10.1111/j.1467-789X.2011.00952.x
- Lee B, Mun S. Association of body mass index and waist circumference with periodontal disease. Oral Health Prev Dent. 2025;23:271-277. doi:10.3290/j.ohpd.c_2017.
- Ding Y, Xu X. Anti-inflammatory effect of exercise training through reducing inflammasome activation-related inflammatory cytokine levels in overweight/obese populations: a systematic review and meta-analysis. Complement Ther Clin Pract. 2022;49:101656. doi:10.1016/j.ctcp.2022.101656
- Gonzalo-Encabo P, Maldonado G, Valadés D, Ferragut C, Pérez-López The role of exercise training on low-grade systemic inflammation in adults with overweight and obesity: a systematic review. Int J Environ Res Public Health. 2021;18(24):13258. doi:10.3390/ijerph182413258
- Chen X, He H, Xie K, Zhang L, Cao C. Effects of various exercise types on visceral adipose tissue in individuals with overweight and obesity: a systematic review and network meta-analysis of 84 randomized controlled trials. Obes Rev. 2024;25(3):e13666. doi:10.1111/obr.13666
- Recchia F, Leung CK, Yu AP, et al. Dose-response effects of exercise and caloric restriction on visceral adiposity in overweight and obese adults: a systematic review and meta-analysis of randomized controlled trials. Br J Sports Med. 2023;57(16):1035-1041. doi:10.1136/bjsports-2022-106304
- Han SJ, Bae KH, Lee HJ, Kim SJ, Cho HJ. Association between regular walking and periodontitis according to socioeconomic status: a cross-sectional study. Sci Rep. 2019;9(1):12969. doi:10.1038/s41598-019-49505-2
- Almohamad M, Krall Kaye E, Mofleh D, Spartano NL. The association of sedentary behaviour and physical activity with periodontal disease in NHANES 2011–2012. J Clin Periodontol. 2022;49(8):758-767. doi:10.1111/jcpe.13669
- Evans PL, McMillin SL, Weyrauch LA, Witczak CA. Regulation of skeletal muscle glucose transport and glucose metabolism by exercise training. 2019;11(10):2432. doi:10.3390/nu11102432
About the Author

Stephen Kelleher, DMD
Stephen Kelleher, DMD, is a periodontist practicing in the greater New York City area, originally from Pittsburgh, Pennsylvania. He earned his DMD from Case Western Reserve University in 2022 and completed his periodontics and implant dentistry training at New York University in 2025. Dr. Kelleher has received several awards recognizing his excellence in periodontics and regenerative dentistry. He is dedicated to evidence-based, patient-centered care with a focus on periodontal therapy, oral tissue regeneration, and implant surgery.