Avoiding complications bonding lithium disilicate

The ability to create a resin cement bond between tooth structure and lithium disilicate has created new possibilities for restorative dentists. Authors have suggested less invasive preparations that will offer the benefits of supragingival margins in the posterior without sacrificing esthetics or retention. (1-4)
MORE ARTICLES BY DR. CHRIS SALIERNO ...
The wrong way to restore an implant
Long-term provisional success for young patients who need implants
I think my implant needs a root canal
The platform is showing! Prosthetic management of implants placed too far coronally
Centric relation mysteries, Part 2: when do we need it?
Centric relation mysteries, Part 1: what is it and how do we find it?
4 ways cloud computing will change dentistry for the better
This author has enjoyed simpler impressions and more hygienic restorative margins using these preparation techniques. However, the more we rely on a resin bond for retention, the more we must ensure that proper insertion protocols are followed.
Common barriers to effective bonding include failure to clean the bonding surfaces and failure to maintain moisture control. The following case illustrates simple techniques used during an insertion visit that will avoid these pitfalls.
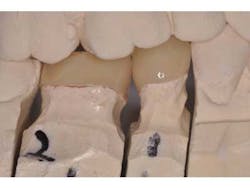
A patient presents with splinted provisional crowns on teeth Nos. 29 and 30 (Fig. 1). The provisionals were splinted to aid retention during the laboratory fabrication phase. The treatment plan called for all-ceramic restorations that could take advantage of resin cement bonding technology, thus the preparation margins were kept supragingival. Lithium disilicate restorations (e.max, Ivoclar) were created monolithically, meaning that no veneering feldspathic porcelain was required (Fig. 2).

After removal of the provisional restorations, the restorations are tried in and assessed for fit. Although this step is necessary, it will contaminate the intaglio surface of the restorations with moisture and bacteria and thus decrease final bond strength.(5) Before application of silane, the intaglio surface should be cleaned with solution to remove any surface contamination before application of silane (Fig. 3). Studies have shown that a proprietary solution (Ivoclean, Ivoclar) is more effective than water or phosphoric acid gel at restoring precontamination conditions of zirconium oxide. (6) An unpublished internal study revealed similar results for lithium disilicate. (7)

Before preparing the tooth surfaces for bonding, it was noted that the interproximal gingival col showed evidence of mild gingivitis (Fig. 4). This is not an infrequent problem, because patients may not maintain the same levels of hygiene around provisional restorations as they would around natural teeth. In this case, the splinted provisional crowns were unable to be flossed and likely contributed to the gingival irritation. A hemostatic paste (Traxodent, Premier) was applied to quell the bleeding (Fig. 5). This paste sets quickly and is able to maintain its position while further steps are taken.


The exposed dentin and enamel surfaces are first treated with a chlorhexidine antibacterial slurry (Conspesis Scrub, Ultradent) to remove residual provisional cement and lower bacterial loads (Fig. 6). This step has been shown to increase the bond strength of adhesive resin cements. (8) After wash and removal of the hemostatic and antibacterial solutions, the area was able to be isolated with dry cotton rolls. If isolation is difficult, the clinician may choose to place a rubber dam. The decontaminated and isolated tooth surfaces are treated with a self-etch primer (Multilink Primer A and B, Ivoclar) (Fig. 7). After drying and light-curing the teeth, the restorations are filled with a dual-cure adhesive resin cement (Multilink Automix, Ivoclar) and seated. Excess cement is removed and the final restorations may be polished (Fig. 8).



Author bio
Chris Salierno, DDS, is a general dentist practicing in Melville, N.Y., and co-editor of Surgical-Restorative Resource™ e-newsletter. He lectures and writes about practice management and clinical dentistry. Additional content is available on his blog for dentists: www.thecuriousdentist.com. You may contact Dr. Salierno by email at [email protected].
References
1.Bakeman EM, Kois JC. Posterior, all-porcelain, adhesively retained restorations. Inside Dentistry. 2009; 5(5):20-30.
2. Helvey GA. Non-retentive, adhesively retained all-ceramic posterior restoration. Inside Dentistry. 2011; 7(2):38-50.
3. Ruiz JL. Supragingival dentistry: Easier and healthier restorative care. Dent Today 2010; 29(3):90-97.
4. Clausen J-O, Abou Tara MA, Kern M. Dynamic fatigue and fracture resistance of non-retentive all-ceramic full-coverage molar restorations. Influence of ceramic material and preparation design. Dent Mater. 2010; 26(6):533-538.
5. Klosa K, Wolfart S, Lehmann F, et al. The effect of storage conditions, contamination modes, and cleaning procedures on the resin bond strength to lithium disilicate ceramic. J Adhes Dent 2009; 11(2):127-135.
6. Wolfart M, Lehmann F, Wolfart S, Kern M. Durability of the resin bond strength to zirconia ceramic after using different surface conditioning methods. Dent Mater 2007; 23(1):45-50.
7. R&D Ivoclar Vivadent AG, Schaan, Liechtenstein, 2011.
8. Sarac D, Bulucu B, Sarac YS, Kulunk S. The effect of dentin-cleaning agents on resin cement bond strength to dentin. J Am Dent Assoc 2008; 139(6):751-758.